You and your partner respond to a downtown office for an
epistaxis call. You find a 35 year old male patient who has had an atraumatic
nosebleed from his left nare for 10 minutes. He seems to be holding pressure on
the anterior part of his nose correctly. He has a pulse of 90 beats per minute,
a respiratory rate of 16, and a blood pressure of 180/100. He is warm and dry without blood on his
shirt, but he explains how severe the bleeding is, with alarming and horrifying
descriptions of “gushing” blood (but no evidence of severe bleeding on him or
in the area). He does not feel like he is swallowing blood. How do you proceed?
Only about 60%
of the population will experience an epistaxis in their lifetime, and 6%
will need medical care to stop the nosebleed. Most cases occur for
children between two and ten years of age and older adults between 50 and 80.
(Those stats surprised me. I’m 42 and get nosebleeds weekly. Who are these 40%
of people who don’t get nosebleeds?!?) Causes of epistaxis include epistaxis
digitorm*, dry air, chronic sinusitis, foreign bodies, intranasal neoplasms, irritant
vapors, rhinitis, trauma, hemophilia, hypertension (maybe; see below),
leukemia, liver disease, anticoagulant use, and thrombocytopenia. The list of
causes is even longer than that. Like with most things, the more benign causes
such as epistaxis digitorum (awesome term!) and dry air are more common.
Unfortunately, that doesn’t help us stratify each specific patient’s relative
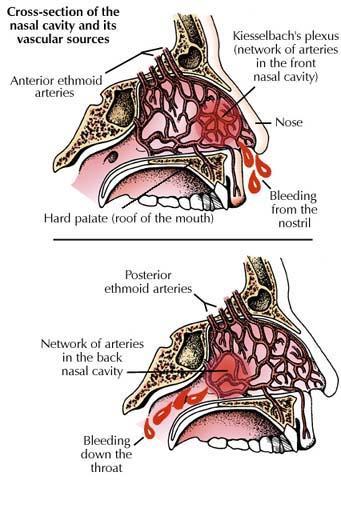
risk. About 90% of nosebleeds come from the anterior nasal septum – an area
called Kiesselbach’s plexus. The other 10% are posterior bleeds that require
emergency department treatment to stop.
 |
| The location of Kiesselbach's plexus in in the anterior septum. This is your target when you're pinching. It involves the soft part of the nose, rather than the nasal bones. Photo source. |
{kind=link}
I deal with epistaxis by starting with the concept of status.
Status epilepticus is defined as a seizure lasting for more than five minutes,
or multiple seizures without fully regaining consciousness in between. But a
seizure can be also regarded as “status” if the patient is still seizing when I
arrive on scene. A similar concept occurs with status asthmaticus – a severe
asthma attack that doesn’t respond to standard treatment. I look at epistaxis
the same way. If I arrive on scene and the patient has been making a reasonable
attempt at stopping the bleeding, I feel
like I can regard the nosebleed as having achieved “status” level: status
epistaxicus. I mean, the nosebleed was bad enough that 911 had to be called,
right? It didn’t respond to normal treatment and it is still going on when I
arrive. Status.
I begin with any needed adjustments to the nose-squeezing
procedure, followed by some quick information collection. I want to know
duration, frequency, estimated blood loss, inciting factors, past medical
history, and so on. To treat the nosebleed, I first get the patient to blow
their nose. Often, ineffective treatment prior to my arrival has created clots
that are difficult to compress and aren’t aiding in hemostasis. So those clots
have to be blown out. Be ready for the bleeding to increase, and have somewhere
for some occasionally giant clots to go.
Next, I spray topical phenylephrine into the nares. A lot of medics
reserve this step for severe, intractable bleeding but I feel like it is appropriate
for any “status epistaxicus” that I come in contact with. Next I pinch the
patient’s nose with my fingers to find the best pressure spot to stop the
bleeding, and then I replace my fingers with a plastic nasal clamp. The timer
starts at that point – fifteen minutes without peeking or loosening the
pressure.
The concept of status epistaxicus is reserved for treatment
decisions, not for transport decisions. Status seizures and status asthma will
generally result in transport. That isn’t true with nosebleeds, of course. If I
can get it stopped and there aren’t other concerns, I usually hope to leave the
patient on scene. Transport is initiated for posterior bleeding (minimal
anterior bleeding, but blood going down the throat, choking on blood, and so on),
large objective blood loss, when the patient is on blood thinners, hypertension
that isn’t decreasing, and if the treatment above fails to stop the nosebleed.
High blood pressure usually isn’t the cause of epistaxis.
Chronic hypertension without effective treatment may cause blood vessels in the
nose to become more fragile, but most experts believe that any hypertension is
the result of the nosebleed rather than the other way around. See, people get
anxious at the sight of blood, especially blood that was recently inside of
them. That anxiety can increase the patient’s blood pressure. Studies rarely
find a cause-effect relationship from hypertension to epistaxis. For example, this
study found that there was “no definite association between epistaxis and hypertension.”
But studies do find a correlation, like here. In the end,
hypertension probably doesn’t cause nosebleed but may prolong
it.
Here
and here are short videos about
Kiesselbach’s plexus and nasal anatomy, including internal views. Enjoy.
* Epistaxis digitorum is a phenomenal way to describe a very
common cause of nosebleed – nose picking. Awesome terminology!
No comments:
Post a Comment